

How Do Surgeons Use FIRE?
FIRE enables surgeons to rapidly, globally, and precisely assess where cancer tissue ends and healthy tissue begins.
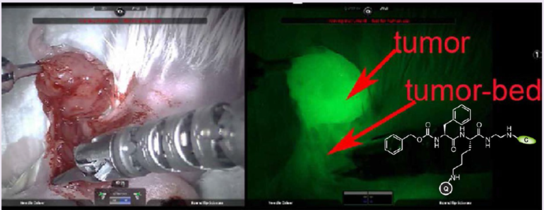
In the Operating Room, the surgeon removes the bulk of the tumor. The surgeon then applies a metered amount of probe into the surgical cavity. After several minutes, the cavity is inspected by a near-infrared camera combined with an excitation source. Images are processed and displayed on a computer in the Operating Room. Any visible glow indicates the presence of active tumor-associated proteases. The surgeon then removes that tissue, reapplies the probe and images again. Iterative slices of tissue may be removed and assessed with the probe until no glow is visible. All tissue resected is passed to pathology for final evaluation.
Why FIRE is a Better Solution
FIRE is a Quenched Activity-Based Probe (qABP)
Unlike other probes, FIRE activates only when it finds active cancer. Other probes may have strong, spurious fluorescent signals which can swamp the signal the surgeon needs to see.
FIRE is Precise
Because it targets only active enzymes found in the margins of cancer—where the tumor is growing most rapidly—FIRE shows surgeons precisely where to cut to remove diseased tissue. Other probes target tumor proteins and can light up the main mass of a tumor, but may miss tumor margins where these proteins are less concentrated.
FIRE is Fast
FIRE activates within minutes of application while the patient is in surgery. Other probes must be given hours or days before surgery or they will not work.
FIRE is Flexible
Most probes are administered systemically. FIRE can be used topically in vivo, topically ex vivo, or they can be used systemically if the surgery requires it.
FIRE is Unique
FIRE’s unique topical administration option requires only minute amounts of probe are sprayed into the patient to find if cancer tissue is present. Other probes require large amounts of probe to be given by IV, raising the risks of toxic or allergic reactions.
Current Applications & Pipeline
FIRE probes are currently in the clinical translation process for the intraoperative assessment of tumor margins for breast cancer and non-melanoma skin cancer. Future applications include brain, lung, and prostate cancers, as well as colon cancer diagnostics.